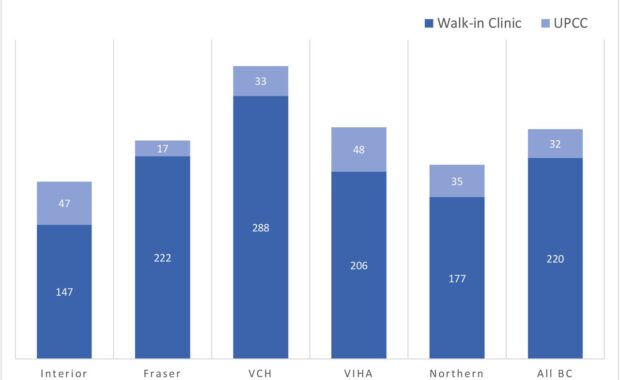
Walk-in clinics are non-hospital based primary care facilities that are designed to operate without appointments and provide increased healthcare

Resolving youth opioid addiction needs evidence-based care
Youth opioid addiction, and related harms continue to rise in North America. With an increasing number of opioid overdoses, there remain significant

Survival of the bitterest: Why dancers are good role models for scientists
What do dance and science have in common? What makes a successful choreographer or scientist? In this post, I speculate about the bitterness of the
Patient-Related Drinking and Alcohol Counselling: Do Doctors Own Lifestyle Habits Matter?
The medical degree isn't a vaccine against addiction. “If you don’t drink as much as your GP, you don't drink too much,” an old saying goes. When
Research Support and Supervisor Development programme: Epidemiologic triad of a successful PhD
The last Friday workshopat University College Dublin addressed a group of twelve supervisors with presentations by an epidemiologist, a physicist, a
Clinical trials are about human dynamics: RCT course in Belfast, May 7-8
As a trialist, the pressure of working on a trial is much bigger than being in a small group educational session. Challenges of implementing a trial
Beg, steel or borrow: getting physicians to recruit patients in clinical trials
Leaflets, adverts and phone calls have all been used to recruit patients in clinical trials with some results. Still, the personal contact remains the
Honor pot: testing doctors’ drug counselling skills in a new pilot study in Ireland
In our new new paper, we outline plans for doing a study which should tell us whether doctors and agonist patients accept psychological interventions
Submitting ethics for new research: killing so many trees
Ethical principles, ethics committees and researchThis has been a busy week from an ethics perspective. All research should be ethical and adhere to